The Australian Medical Student Journal: a nationwide endeavour
Welcome to Volume 4, Issue 1 of the Australian Medical Student Journal. This issue of the AMSJ continues to develop our core aims of supporting medical student research by providing …

Welcome to Volume 4, Issue 1 of the Australian Medical Student Journal. This issue of the AMSJ continues to develop our core aims of supporting medical student research by providing …
Early last year, a David and Goliath battleraged between the most unlikely of foes. The gripes of a single blog post inspired a group of disaffected mathematicians and scientists to …

“Make up your mind how many doctors a community needs to keep it well. Do not register more or less than this number.’’ George Bernard Shaw If you have ever …

The conception of dizygotic twins is a complex trait. It is thought to be influenced by a variety of environmental and genetic factors and displays significant regional variation in prevalence …
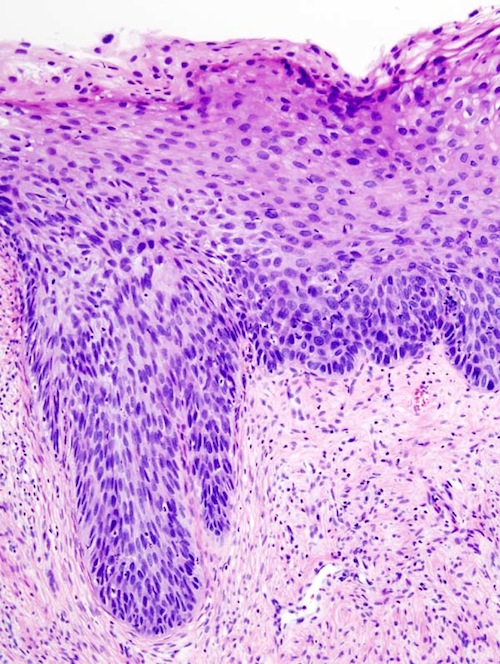
Vulval intraepithelial neoplasia (VIN) is a condition which is increasingly prevalent, particularly in young women, [1] but is a topic rarely touched upon in medical school. The following article reviews …

Pertussis, or whooping cough, is a potentially fatal respiratory illness caused by the Bordetella pertussis bacteria. It commonly occurs in infants who have not completed their primary vaccination schedule. [1] …

Effective and efficient methods of learning are important for medical students to tackle the plethora of information available. A technique that is gaining increasing popularity is Spaced Repetition Learning. Spaced …

“Our right to take back responsibility.” Noel Pearson, 2000 [1] This emotive aphorism by Pearson embodies the struggle of Australia’s Indigenous people to gain control of their destiny, which for …
Jayasinghe, S. Rohan. ECG Workbook, Australia: Elsevier; 2012. RRP: $59.95 This is an Elsevier supported book review Like tools are to a plumber, correct ECG interpretations are to a doctor. …
Background: Human papillomavirus (HPV) is a family of highly contagious sexually transmitted viruses which are associated with the development of genital warts and certain HPV related cancers in males and females. …