Background: Abusive Infant Head Trauma (AIHT) is preventable, but there are few reviews of interventions to prevent AIHT. In the Australian health system context, only one review of AIHT was found. Its primary focus was to raise awareness of AIHT, detailing AIHT incidence and outcomes, but only briefly touching on prevention. [1] This literature review attempts to fill this gap by providing the findings of a systematic search of available studies of AIHT prevention programs and approaches at the primary, secondary, and tertiary level, which may be applicable in Australian settings. Methods: International peer-reviewed journal articles were systematically searched via MEDLINE-Ovid and PubMed databases. All papers that were not original research and were not published after the year 2000 were excluded from this review. Original research was further classified into intervention research, descriptive, and measurement research. The quality of intervention research studies was assessed using two assessment tools: EPHPP (quantitative studies) and CASP (qualitative studies). Results: The search found 50 papers. Thirty-two did not meet inclusion criteria, leaving a total of 18 original research papers. Eight were intervention research (three strong, one moderate, and four weak), ten were descriptive research, and there were no measurement studies. Conclusion: The key to AIHT prevention is through universal primary prevention, with education increasing knowledge in parents and healthcare practitioners. Of the studied programs, the Period of PURPLE Crying Program© has been shown to be the most effective. However, further studies are required to assess the relevance of this program in Australian settings.
Background
Abusive Infant Head Trauma (AIHT) has significant morbidity and mortality outcomes. [2,3] Violent, manual shaking of an infant causes rapid and repetitive acceleration-deceleration and rotation of the head, leading to vascular and neural injuries. [2] Neurologic disability occurring in survivors can include cognitive, motor, visual, and behavioural disturbances. [2,4-6] Infants may also present with variable fractures including fractures of long bones, ribs, or vertebrae. [5] Identifying injuries of AIHT can result in children being removed from parents, loss of parental rights, and imprisonment. [4] In Australia, AIHT incidence has been estimated as 29.6 cases per 100,000 infants; this is based on hospitalised cases only. [3]
The peak incidence of AIHT occurs in the second month of life and corresponds to the normal development of increased crying in the infant. [7,8] Prolonged and inconsolable crying is reported as the most common trigger. Parents are the most common agents of infant shaking. [4,5,7,9] Therefore, AIHT is a good candidate for the development of a prevention strategy, with parents being the risk group and crying being the stimulus.
Evidence indicates that AIHT is preventable. [2,9-14] Efforts to find effective prevention strategies have increased with the growing recognition of AIHT’s clinical symptoms, its prevalence, and devastating consequences. [4] AIHT prevention strategies include primary, secondary, and tertiary methods. [9] By systematically searching and providing a summary of available research, this literature review aims to highlight what we do and do not know about AIHT prevention thereby increasing the awareness of AIHT in medical professionals and encouraging implementation of prevention programs in Australian healthcare settings.
Methods
International peer-reviewed journal articles were systematically searched via MEDLINE-Ovid and PubMed databases using the search terms: “shaken baby syndrome”, “shaken baby syndrome prevention”, “infant abusive head trauma”, and “period of purple crying program”. Article titles and abstracts were searched for AIHT prevention interventions. This search resulted in 50 articles, which were further analysed and classified. All review articles, program descriptions, discussion papers, commentaries, case reports, and literature published prior to the year 2000 were excluded from the search results. Original research published from 2000 was included in the review. The start date designated for the search was determined by the timeframe when prevention strategies were developed and researched (in the early 2000s). [9]
The quality of intervention research was then analysed using the Effective Public Health Practice Project assessment tool (EPHPP) for quantitative research, [16] and the Critical Appraisal Skills Programme tool (CASP) for qualitative research. [17] Consistent with the purpose of the appraisal tools to assess the effectiveness of public health programs and interventions, the quality of only intervention research studies that evaluate what works was assessed. The EPHPP Quality Assessment Tool sections A to F (A. selection bias; B. study design; C. confounders; D. blinding; E. data collection methods; F. withdrawal and drop-outs) were coded strong, moderate, or weak according to the rating scale of the EPHPP dictionary. For qualitative studies, the CASP quality assessment tool was used to assess the clarity of study objectives, methodological quality, research design, data collection and analyses, ethical considerations, clarity of the statement of findings, and the value of the research. To assess the study quality of those using mixed-methods study design, the qualitative and quantitative components were assessed separately using both of the aforementioned tools.
Results
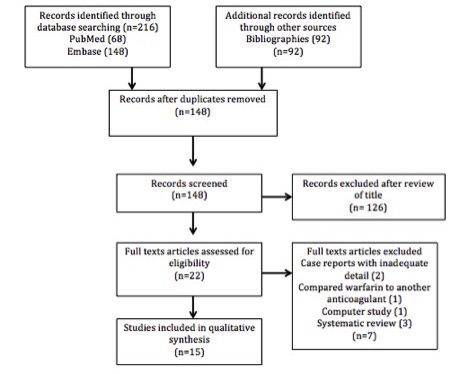
The search resulted in 50 articles. Of these, 32 were excluded as not being original research published after the year 2000, leaving a total of 18 original research papers. Of these, only 8 were intervention research studies, 10 were program descriptions, and there were no measurement research studies (Figure 1).
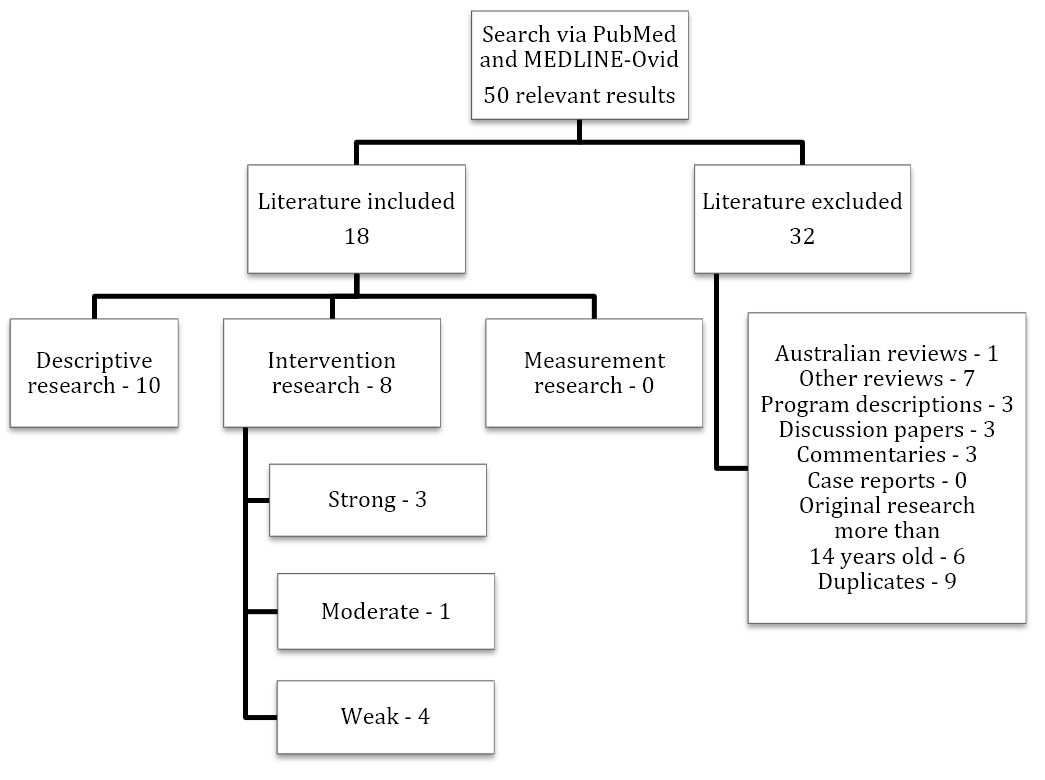
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of search results. This diagram shows the flow of information through the different phases of the systematic search. It depicts the number of articles found, included, and excluded, and the reasons for exclusions.
<<Insert Figure 1>>
Applying the quality appraisal criteria resulted in assessments of the eight intervention studies. Three were rated strong, one moderate, and four weak (Table 1).
Table 1: AIHT intervention quantitative studies assessed using EPHPP.
| Study | Selection bias | Study design | Confounders | Blinding | Data collection method | Withdrawal and drop-outs | Results |
| Barr et al. 2009a | Strong | Strong | Strong | Strong | Moderate | NA | Strong |
| Barr et al. 2009b | Strong | Strong | Strong | Strong | Strong | NA | Strong |
| Altman et al. 2011 | Moderate | Moderate | Weak | Weak | Moderate | Weak | Weak |
| Dias et al. 2005 | Strong | Strong | Strong | Strong | Moderate | N/A | Strong |
| Shephard et al. 2000 | Weak | Weak | Weak | Weak | Weak | Strong | Weak |
| Stewart et al. 2011 | Moderate | Weak | Weak | Weak | Moderate | Weak | Weak |
| Goulet et al. 2009 (quantitative component) | Moderate | Weak | Weak | Weak | Weak | Weak | Weak |
| Russell et al. 2008 | Weak | Moderate | Weak | Moderate | Weak | Strong | Moderate |
Table 2: Qualitative studies assessed using CASP.
| Study | Study objectives | Methodological quality | Research design | Data collection and analyses | Ethical considerations | Statement of findings | Value of the research |
| Goulet et al. 2008 (qualitative component) | Clearly stated | Appropriate | Appropriate | Poor | Ethically approved | Clearly stated | Valuable |
Discussion
The review of the available literature indicates that there is little evidence about what works to prevent or treat AIHT, and more than half of the intervention studies were of poor quality.
Primary prevention studies
Two of the strong intervention studies were randomised controlled trials conducted by Barr et al. (2009a, 2009b). They were studies of a universal primary prevention program of AIHT that targeted parents of infants and newborns, and sought to prevent shaking from occurring through education. [10,11] The prevention program was called the Period of PURPLE Crying program (PURPLE©) produced by the National Center of Shaken Baby Syndrome (Utah, USA). [4,5,8-12,14] PURPLE© stands for Peak of crying, Unpredictable crying that has no apparent reason, Resists soothing, Pain-like face, Long-lasting crying for 30 to 40 minutes or longer, and Evening crying. [10,14] The program included a ten-minute DVD and an eleven-page coloured booklet, targeting all parents of newborns. It was an evidence-based program delivered in three instalments that used 25 years of research on normal infant crying to educate parents on crying characteristics, coping strategies, and the dangers of shaking. [14]
The two studies by Barr et al. found that administration of the PURPLE© materials had led to statistically significant improvements in maternal knowledge and behaviour relevant to shaking, compared to control material. Compared to mothers that received the control materials, for mothers who received the PURPLE© program, knowledge about normal infant crying was 5% higher in the first study and 6% higher in the second study. [10,11] Sharing information was shown to be higher in mothers who received the PURPLE© program than those who received the controls; there was an 8% increase in sharing descriptions of crying, 13% increase in advice about walking away when frustrated, and 13% increase in warnings about the dangers of shaking. [10,11]
The strong intervention study by Dias et al. indicated that a universal hospital-based parent education program regarding the dangers of violent infant shaking, delivered prior to an infant’s discharge, significantly reduced the incidence of AIHT. All hospitals that provided maternity care in an eight-county region of western New York State were asked to provide parents with information describing the dangers of violent infant shaking and alternative responses to persistent infant crying. Program compliance was assessed by documenting the number of voluntary commitment statements signed by parents affirming their receipt and understanding of the materials, and returned by participating hospitals. Parents’ recall of the information was assessed by follow-up telephone interviews conducted with 10% of parents, seven months after the child’s birth. Finally, the regional incidence of AIHT was contrasted with the incidence during the six preceding years, and with statewide incidence rates during the study period. The study found a high voluntary compliance with the program, high recall of the information, and a decrease in AIHT by 47% amongst participating families during the six-year study, with no comparable decrease in the state. [9]
A weak retrospective descriptive study by Stewart et al., found that the three instalments of the PURPLE© program were crucial to AIHT prevention. Stewart et al. compared patients presenting with cases of AIHT that presented to the London Children’s hospital (London, UK) from 1991 to 2010. Pre-trained maternity nurses delivered the program to parents. Stewart et al. found a 47% increase in the knowledge of nurses on crying, post-PURPLE© training, and 78% said it would be easy to incorporate into their daily work schedule. Instalment one involved the DVD and booklet. Stewart et al. (2011) stated only 6.3% of families did not receive the program in the hospital, and needed to be educated during their home visits. [14] Instalment two was a reinforcement of the message delivered by a health nurse home visitor, paediatrician, family doctor, or other health practitioner at a public health clinic. It involved simply discussing with the parents the concepts taught in the program and giving parents a copy of the program if they had not collected one at the hospital. Instalment three was a public education campaign. It provided information to the general public in an attempt to educate people in society more generally about inconsolable infant crying and the dangers of shaking. [10,11] Altman et al. conducted a weak intervention study showing that hospital-based parent education, delivered to all those with newborns, could significantly reduce the risk of sustaining an abusive head injury induced by shaking. [12] Further studies are required to gain evidence of the PURPLE© program’s effects on reducing the incidence of AIHT in Australia.
Literature available on AIHT prevention programs other than PURPLE© was extremely limited. A moderate-strength study conducted by Russell et al. (2008), compared types of AIHT prevention material. [13] The results showed that material delivered digitally via DVD, particularly material demonstrating alternative behaviours, was more successful in transferring awareness than interventions that involved only a brochure. DVDs significantly increased the potential for improving the population’s awareness of AIHT. This study was not specific for the period of PURPLE© crying program DVD, and suggests that digital footage that is Australian-focused may be utilised equally as effectively. [13] Parents watched the DVD in the hospital before taking it home with their newborn. The nurse recommended to parents that they review the materials at home, and share the information with other caregivers of their baby. [10,11]
In a weak intervention study, Shephard et al. found the “Don’t Shake the Baby” education package was helpful to the majority of mothers; 49% said that they were less inclined to shake their babies after reading it, and 91% said they thought other parents should receive the same information. [18] The package involved brochures and cards with suggested coping strategies during inconsolable, frustrating crying, and information on the dangers of shaking; as well as television and radio public service announcements and posters containing information about AIHT. [18] These materials could be adapted to suit different language and cultural groups.
Goulet et al. analysed the adequacy and relevance of the Perinatal Shaken Baby Syndrome Prevention Program (PAIHTPP) based on parental and nurse feedback in another weak intervention study. [2] The PAIHTPP used educational cue-cards to increase knowledge about infant crying, triggering of caregiver frustration, and its potential progression to shaking, while suggesting coping strategies for frustration. [2] Findings indicated PAIHTPP to be relevant in all birthing institutions involved in the study. [2] The majority of birthing institutions reported increased knowledge about infant crying, anger, coping strategies, and AIHT. [2]
Other AIHT prevention programs that are available, which have not been evaluated, include programs specific for fathers, especially fathers in the military, prison and youth halfway houses, and programs specific for high school students. The programs are educational and contain appropriate language and imagery for the target audience. [19]
Secondary prevention studies
Secondary prevention programs target specific subsets of the population considered to be at higher risk for child maltreatment. [8] It has been found that an increase in parental or caregiver stress correlates with an increase in AIHT incidence. [2,14,20] Therefore, parents and carers categorised as being under stress can be targeted for secondary prevention programs. Parents who may be under increased stress include single parents, young parents, those that are drug-dependent, alcohol-dependent, have impulse disorders, control problems, low socioeconomic status, or isolated parents. [14,20] Stewart et al. indicated that geographical areas that may be at higher risk for AIHT should be targeted for extra advertising campaigns, specifically those delivered in instalment three of the PURPLE© program. [14] However, studies indicate that the focus of prevention should be primary and universal [10-13]; studies about secondary prevention programs were approximately 20 years old, and as such have not been included in this review. [21,22]
Tertiary prevention studies
Children who have been shaken and diagnosed with AIHT are targeted by tertiary prevention programs, which aim to prevent progression of injury and recurrence in the child affected and or other siblings. Diagnosis of AIHT is required before tertiary prevention can be implemented. Diagnosing AIHT is difficult due to its non-specific presenting symptoms and vague explanations made by perpetrators. [6] Reporting suspicion of shaking to departments of child protection can prevent further abuse to the child. [4,6]
According to research by King et al., the common clinical manifestations of AIHT are subdural effusion, retinal hemorrhages and cerebral oedema. [6] Cerebral oedema can be reduced through pharmacotherapy such as glucocorticoids, hyperosmotic agents, diuretics, and sedative-anesthetic agents to prevent progression of neurological damage. [15,23-25] Tertiary prevention through child protection case management is not specific to AIHT, but rather is managed like all traumatic brain injuries in children, through rehabilitation.
Conclusion
Literature on AIHT prevention is limited. Quality research in this area is needed because of the limited number of articles available, more than half of which are of limited quality. This review identified three qualitatively strong intervention studies, one moderate, and four weak, as well as ten program-description studies. These studies indicate that AIHT can be prevented through universal primary prevention techniques. These must be educational and ideally involve the use of a DVD in addition to written materials. Of the studied programs, the Period of PURPLE Crying Program© has been shown to be the most effective. Tertiary prevention programs through case management by child protection agencies aim to restore child function and prevent progression of neural damage through rehabilitation, and to prevent reoccurrence by legal investigation of the perpetrator. However, further studies are required to assess its impact on AIHT incidence. In particular, evaluation is needed of the relevance of the American-developed Period of PURPLE Crying program© in Australian settings.
This article is dedicated to Baby Joseph. Joseph did not receive any benefit from primary prevention efforts, and the effects of secondary and tertiary efforts to ameliorate the harm from his allegedly repeated shaking experiences have been limited and are ongoing. His prognosis is guarded, and a return to his premorbid level of function is unlikely. His case illustrates a great gulf between what is known about primary prevention and what is currently practised as primary prevention in most of Australia. Joseph’s situation is sadly and predictably, not unique. Primary prevention programs may lead to better baby outcomes into the future.
Acknowledgements
I wish to acknowledge public health researcher, Associate Professor Janya McCalman for mentoring me through the systematic review process and editing the paper. I wish to also thank rural generalist medical practitioner, Dr Bill Liley, who has mentored me through my medical degree, and who has a particular interest in preventing Shaken Baby Syndrome. Thanks also to the Commonwealth Government for funding my medical studies through a Remote Area Medical Undergraduate Scholarship.
Conflicts of interest
None declared.
References
[1] Liley W, Stephens A, Kaltner M, Larkins S, Franklin RC, Tsey K et al Infant abusive head trauma: incidence, outcomes and awareness. Aust Fam Physician. 2012;41(10):823.
[2] Goulet C, Frappier JY, Fortin S, Déziel L, Lampron A, Boulanger M. Development and evaluation of a shaken baby syndrome prevention program. JOGNN. 2009;38(1):7-21.
[3] Kaltner M. Abusive head trauma: incidence and associated factors in Queensland [PhD thesis]. Brisbane, Qld: University of Queensland; 2010.
[4] Christian CW, Block R. Abusive head trauma in infants and children. Pediatrics. 2009;123(5):1409-11.
[5] American Academy of Paediatrics: Committee on Child Abuse and Neglect. Shaken baby syndrome: rotational cranial injuries—technical report. Pediatrics. 2001;108:206–10.
[6] King WJ, MacKay M, Sirnick A. Shaken baby syndrome in Canada: clinical characteristics and outcomes of hospital cases. Can Med Assoc J. 2003;168(2):155-9.
[7] Talvik I, Alexander RC, Talvik T. Shaken baby syndrome and a baby’s cry. Acta Paediatr. 2008 June;97(6):782–5.
[8] Barr RG, Trent RB, Cross J. Age-related incidence curve of hospitalized shaken baby syndrome cases: convergent evidence for crying as a trigger to shaking. Child Abuse Neglect. 2006;30(1):7-16.
[9] Dias MS, Smith K, Mazur P, deGuehery K, Li V, Shaffer M. Preventing abusive head trauma among infants and young children: a hospital-based, parent education program. Pediatrics. 2005;115(4):470-7.
[10] Barr R, Rivara F, Barr M, Cummings B, Taylor J, Lengua L et al. Effectiveness of educational materials designed to change knowledge and behaviors regarding crying and shaken-baby syndrome of newborns: a randomized, controlled trial. 2009;123(3):972-80.
[11] Barr RG, Barr M, Fujiwara T, Conway J, Catherine N, Brant R. Do educational materials change knowledge and behavior about crying and shaken baby syndrome? A randomized controlled trial. 2009;180(7):727-33.
[12] Altman RL, Canter J, Patrick PA, Daley N, Butt N, Brand D. Parent education by maternity nurses and prevention of abusive head trauma. Pediatrics. 2011;128(5):1164-72.
[13] Russell BS, Trudeau J, Britner PA. Intervention type matters in primary prevention of abusive head injury: event history analysis results. Child Abuse Neglect. 2008;32(10):949-57.
[14] Stewart TC, Polgar D, Gilliland J, Tanner D, Murray G, Parry N et al. Shaken baby syndrome and a triple-dose strategy for its prevention. J Trauma Acute Care Surg. 2011;73(6):1801-7.
[15] Papangelou A, Lewin III JJ, Mirski MA, Stevens R. Pharmacologic management of brain edema. Current Treat Option N. 2009;11(1):64-73.
[16] McMaster University. Effective public health practice quality assessment tool for quantitative studies, 2008, McMaster University School of Nursing: Canada.
[17] Network, C.I. Critical Appraisal Skills Programme: Making sense of evidence about clinical effectiveness: qualitative research studies. 2010.
[18] Shepherd J, Sampson A. Don’t shake the baby’: towards a prevention strategy. Brit J Soc Work. 2000;30(6): 721-35.
[19] Bechtel K, Le K, Martin, KD. Impact of an educational intervention on caregivers’ beliefs about infant crying and knowledge of shaken baby syndrome. Acad Pediatr. 2011;11(6):481–6.
[20] Keenan HT, Runyan DK, Marshall SW, Nocera MA, Merten DF, Sinal SH. A population-based study of inflicted traumatic brain injury in young children. JAMA. 2003;290(5):621-6.
[21] Olds D, Henderson CR, Chamberlin R, Tatelbaum R. Preventing child abuse and neglect: a randomized trial of nurse home visitation. Pediatrics. 1986;78(1):65–78.
[22] Olds D, Eckenrode J, Henderson CR, Kitzman H, Powers J, Cole R. Long-term effects of home visitation on maternal life course and child abuse and neglect: 15year follow-up of a randomized trial. JAMA.1997;278(8):637–43.
[23] Galicich JH, French LA, Melby JC. Use of dexamethasone in treatment of cerebral edema associated with brain tumors. Lancet, 1961;81:46-53.
[24] Knapp JM. Hyperosmolar therapy in the treatment of severe head injury in children: mannitol and hypertonic saline. AACN .Clin Issues. 2005;16(2):199-211.
[25] Rhoney DH, Parker D. Use of sedative and analgesic agents in neurotrauma patients: effects on cerebral physiology. Neurol Res. 2001 Mar-Apr;23(2-3):237-59.