For Euthanasia: Murder versus mercy
Under existing law, if a doctor intentionally and compassionately hastens a patient’s death, upon the patient’s request to end their suffering, that doctor can be prosecuted with the most serious …

Under existing law, if a doctor intentionally and compassionately hastens a patient’s death, upon the patient’s request to end their suffering, that doctor can be prosecuted with the most serious …

There is so much misinformation and outdated information surrounding the debate about assisted dying that it is important to try to ascertain what evidence is currently available. Otherwise, myths tend …
The issue of assisting or hastening death is not a new phenomenon. In the 5th century BC, Hippocrates explicitly stated that new physicians must refrain from such a practice. [1] …
I wish to make several points in response: Relief of suffering My colleague claims that with ‘expert’ palliation ‘symptoms can be relieved, explanations can be given and suffering can be …

About AMSA The Australian Medical Students’ Association (AMSA) is the peak representative body for medical students in Australia. AMSA connects, informs and represents students studying at each of the 20 …
This report describes a case of a 33-year-old female with cyclical vomiting associated with cannabis use, which was subsequently diagnosed as Cannabinoid Hyperemesis Syndrome (CHS). While the exact epidemiology of …
Pericardial effusions are not uncommonly encountered, and can be of infectious, autoimmune, malignant, and idiopathic aetiology. Large pericardial effusions may result in cardiac tamponade, which is a medical emergency. We …
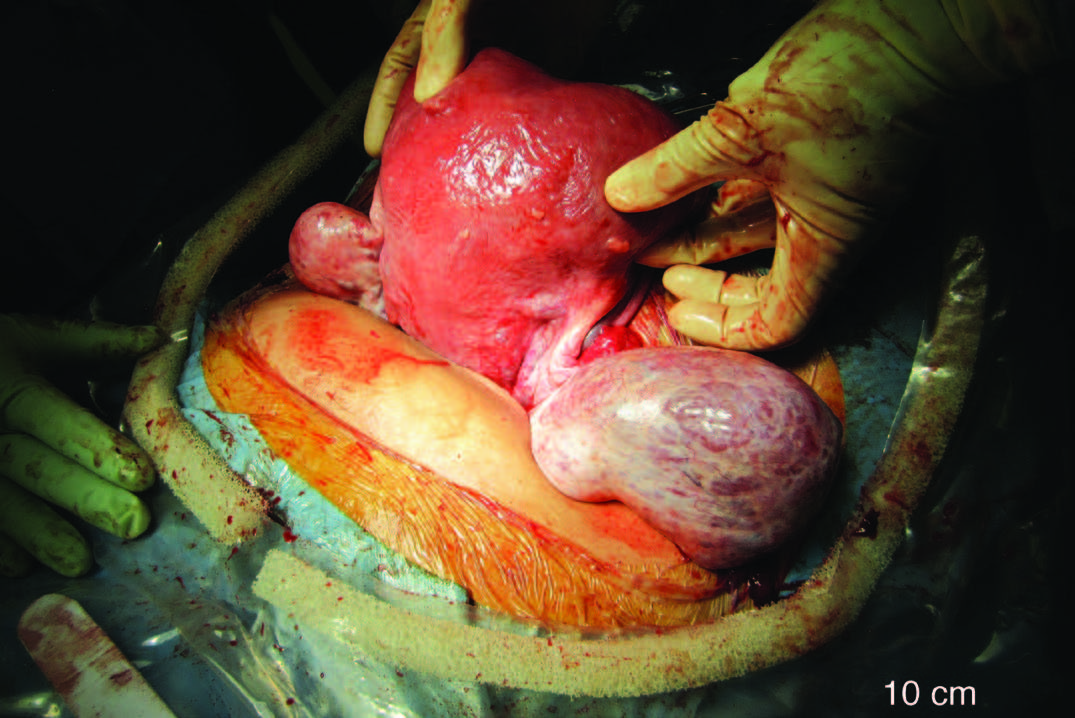
A 33 yr old woman presents with irregular menstrual bleeding and on examination has bilateral adnexal masses. At this original presentation, she was unexpectedly pregnant in the first trimester. Throughout …

Background: The clavicle is one of the most commonly fractured bones in the body. Interns are often delegated to treat these cases in an emergency department. This audit looks at …
Choosing a method of pain relief for childbirth is an extremely personal, and often well-considered, decision. For many women, childbirth is the most painful experience they will ever encounter. It …